
Case Report | DOI: https://doi.org/10.31579/2690-1919/159
1 Radiology Department, Usmanu Danfodiyo University, Sokoto.
2 Radiology Department, Gombe State University, Gombe.
3 Radiology Department, Usmanu Danfodiyo University Teaching Hospital, Sokoto.
*Corresponding Author: SULE Muhammad Baba, Department of Radiology, Usmanu Danfodiyo University, Sokoto.
Citation: Sule MB, Umar AU, Gele IH, Yisa CB, Bilyaminu U, et al (2021). Self-Medication -An Intensifying Global Concern. J Clinical Research and Reports, 7(4); DOI:10.31579/2690-1919/159
Copyright: © 2021 SULE Muhammad Baba, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 March 2021 | Accepted: 14 April 2021 | Published: 26 April 2021
Keywords: ultrasonography; schistosomiasis; urinary bladder; hydroureteronephrosis; pelvi-calyceal; praziquantel; parasitology
Urinary schistosomiasis (US) causes chronic ill health and caused by the blood fluke Schistosoma haematobium. This disease is endemic in Africa and eastern Mediterranean countries, and has a predilection for the male gender.
This is a 64-year-old farmer (swampy farming and fishing) for more than forty years, that was referred from a peripheral health care centre for abdominal and pelvic ultrasonography on account of abdominal pain and discomfort, bilateral loin pain, dysuria, and terminal hematuria for close to a year duration of onset.
The ultrasonography demonstrated bladder wall thickening, mucosal thickening and polypoid proliferation in to the bladder lumen, irregular echogenic crust in the bladder base, suspended mobile echoes in urine most likely from hematoma and/or cystitis, there is associated mild-moderate biliterate dilatation of the pelvi-calyceal systems and ureters(hydroureteronephrosis). The remaining abdominal and pelvic organs appeared normal.
Urinary parasitology demonstrated the ova of Schistosoma haematobium confirming the diagnosis of urinary schistosomiasis.
We report the ultrasonographic features of urinary schistosomiasis because of its peculiar presentation and to emphasize importance of ultrasound in its assessment.
Urinary schistosomiasis is mainly caused by Schistosoma haematobium especially in endemic areas, the sites of predilection are the bladder, lower ureters, urethra, seminal vesicles, cervix, and vagina [1].
Following deposition of the ova from Schistosoma at predilection sites, this initiates granuloma formation and coalesce to form pseudotubercles appearing as seed-like bodies with circumferential zone of hyperemia; seen in early and active disease. The late presentation is the sandy patch; these are calcified ova beneath the atrophic mucosa appearing like sand giving the mucosa a ground-glass appearance [1,2].
The world Health Organization (WHO), in 1996, estimated that about 200 million individuals were affected by schistosomiasis worldwide, and most are rural dwellers, about 20 million of these were severely affected by the disease and another 120 million were symptomatic with the disease [3,4].
Schistosomiasis is endemic in sub-Saharan African most especially Nigeria, the burden of the disease is estimated at about 29 million cases, with varying cases of both urinary and intestinal cases across the country, though the cases of urinary infection appear prevalent [5,6].
Schistosomiasis has predilection for the male gender most likely occupationally inclined, following exposure to infected water from swimming, fishing and other agricultural activities. The prevalence and severity of the disease appears more in children and adolescent [7,8].
Schistosomiasis often present with varying features especially among the male gender, these are loin pain, terminal hematuria, hemospermia, dysuria, lower abdominal pain [1,3,9].
The diagnosis of schistosomiasis is made by detection of the parasite ova in stools, urine, and biopsy specimens from affected organs, or presence of antibodies to the different stages of the parasite or antigens circulating in the body fluids by serologic techniques [10,11].
Radiological imaging also plays role in the diagnosis of urinary schistosomiasis, these are basically ultrasonography, Doppler studies, plain radiography, computed tomographic scan (CT), cystoscopy and magnetic imaging resonance (MRI) [1,10,12].
The treatment of urinary schistosomiasis is widely done by administration of oral praziquantel in a dose of about 40mg per body kilogram as a single dose, other regimen which include metrifonate and artemisinin have been also used, though praziquantel happens to be widely accepted and most efficacious [1,13].
This is a 64-year-old farmer (swampy farming and fishing) for more than forty years, that was referred from a peripheral health care centre for abdominal and pelvic ultrasonography on account of abdominal pain and discomfort, bilateral loin pain, dysuria, and terminal hematuria for close to a year duration of onset.
The patient is conscious and alert and well oriented, not pale, anicteric, acyanosed, no finger clubbing and not in painful distress and no pedal edema or swelling of any body part currently.
The patient had a blood pressure of about 120/70mmHg, pulse rate was 72 beats per minute and a respiratory rate of about 12cycles per minute.
The blood electrolytes were normal, blood urea was also normal (12milligram per deciliter) and blood creatinine level was also normal (1.1milligram per deciliter of blood), the packed cell volume was about 38% and the erythrocyte sedimentation rate was 7mm/hr. the white blood cell count was elevated and about 13500 white blood cells per microliter.
Urine analysis demonstrated pus cells, and blood cells, no protein nor glucose was demonstrated in the urine sample.
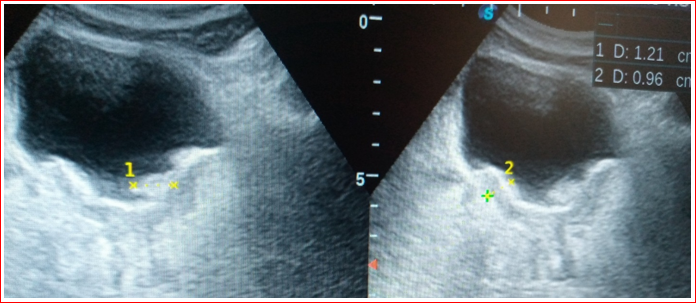
The ultrasonography demonstrated a bladder appearing contracted with diminished capacity, bladder wall thickening of about 9.6mm, mucosal thickening and polypoid proliferation (measuring about 12.1mm in diameter) in to the bladder lumen, irregular echogenic crust in the bladder base, suspended mobile echoes in urine most likely from hematoma and/or cystitis (all in figure 1), there is associated mild-moderate biliterate dilatation of the pelvi-calyceal systems (figure 2) and ureters; the hydroureteronephrosis. The remaining abdominal and pelvic organs appeared normal.

Urinary parasitology demonstrated the ova of Schistosoma haematobium confirming the diagnosis of urinary schistosomiasis.
The patient was administered with oral praziquantel in a dose of 40mb/body kilogram, he had a first course to repeat the parasitology after two-weeks, he was also advised on good personal health and hygienic practices, and to come for a follow-up visit in two-weeks.
Urinary schistosomiasis is a tropical infection caused by Schistosoma haematobium, regarded as part of the neglected Tropical diseases with high incidence across African continent affecting more than 200 million people [14]. The case under review is of the African descent, living in an African country with Schistosoma Haematobium detected in his urine sample, thereby conforming to this literature.
Schistosomiasis has predilection for the male gender most likely occupationally inclined, following exposure to infected water from swimming, fishing and other agricultural activities. The prevalence and severity of the disease appears more in children and adolescent [7,8]. The case under review is a male, a fisherman and farms in a swampy land for almost forty years, thereby conforming to these literatures.
Schistosomiasis is endemic in sub-Saharan African most especially Nigeria, the burden of the disease is estimated at about 29 million cases, with varying cases of both urinary and intestinal cases across the country, though the cases of urinary infection appear prevalent [5,6]. The index case lives in Nigeria, a sub-Saharan country with features of urinary schistosomiasis, thereby conforming to these literatures.
Schistosomiasis often present with varying features especially among the male gender, these are loin pain, terminal hematuria, hemospermia, dysuria, lower abdominal pain [1,3,9]. The case under review also presented with dysuria, hematuria, lower abdominal pain and discomfort. Thereby conforming to these literatures.
Patients with schistosomiasis often present with secondary bacterial infection, in adults, hematuria may disappear, with evolvement of fibrosis, calcification, hydroureteronephrosis, eventual renal failure, with chronicity squamous cell carcinoma may also occur [12,14]. The index case had hematuria, echogenic crust most likely calcification, fibrosis, hydroureteronephrosis, but no evidence of renal failure and malignant transformation as at the time of this report.
Radiological imaging also plays role in the diagnosis of urinary schistosomiasis, these are basically ultrasonography, Doppler studies, plain radiography, computed tomographic scan (CT), cystoscopy and magnetic imaging resonance (MRI) [1,10,12]. The index case had ultrasonography with Doppler interrogation, these demonstrated varying changes in the bladder and urinary tracts, the Doppler showed increased vascularity in the bladder wall/mucosa. These agrees with the above literatures.
Ultrasonography is vital in assessing cases of urinary schistosomiasis in detecting the disease and the severity, this demonstrates varying degree of bladder and ureteric and renal affectation of schistosomiasis most commonly wall thickening with hydroureteronephrosis [15-18]. The patient had ultrasonography, this demonstrated a bladder that appear contracted with circumferential wall thickening more in the base, mucosal thickening and protrusion in to the lumen, presence of irregular echogenic crust in the base with associated suspended mobile echoes in urine. Bilateral mild-moderate hydroureteronephrosis was also demonstrated in this patient. Thereby agreeing to these literatures.
The treatment of urinary schistosomiasis is widely done by administration of oral praziquantel in a dose of about 40mg per body kilogram as a single dose, other regimen which include metrifonate and artemisinin have been also used, though praziquantel happens to be widely accepted and most efficacious [1,13]. The case under review had a course of praziquantel in a dose of 40mg/kg, thereby conforming to these literatures.
Schistosomiasis is endemic in Africa, and most times occupational related, individuals with high risk should be monitored adequately by urine parasitology and ultrasonography to prevent occurrence of schistosomiasis among these subjects thereby reducing the morbidity and complication of malignant transformation amongst them.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
